
Prevent CT and MRI Scan Missed Diagnoses: Get Answers the First Time
Dealing with unexplained, persistent pain can be exhausting, especially when diagnostic tests fail to provide clear answers. Rigid imaging protocols can create clinical tunnel vision and lead to missed diagnoses on CT and MRI scans. When this happens, important adjacent findings may be overlooked, resulting in unresolved symptoms, delayed treatment, added expense, repeat radiation exposure from CT, and duplicate diagnostic charges for MRI.
In this blog, we explain why these diagnostic gaps occur and how a more adaptable approach can help ensure a complete diagnosis the first time.
Key Takeaways
- Strict scan boundaries can cause important findings outside the prescribed field to be overlooked.
- Incomplete imaging may lead to unnecessary repeat scans, extra costs, and additional radiation exposure from CT and duplicate charges for MRI.
- Patients can reduce the risk of missed findings by clearly sharing all symptoms and confirming the exact scope of the scan.
Quick answer: Rigid imaging boundaries can lead to missed diagnoses, but sharing complete symptom information and choosing an adaptable imaging team can improve accuracy on the first visit.

What is a Missed Diagnosis in Medical Imaging?
When people hear “missed diagnosis,” they often think of a broken CT or MRI machine or a radiologist misreading the study. In reality, it is usually more about limited scanning scope and inflexible protocols.
Referring clinicians order scans to answer a specific clinical question, and scans are performed within a defined field of view. Disease, however, does not always stay within those boundaries. If the actual cause of pain lies just outside the intended area, it may be overlooked simply because it was not the original focus of the study.
At its core, a missed diagnosis occurs when the medical team does not gather enough information to see the full picture. For example, an abdominal CT for severe stomach and back pain may show normal abdominal organs but miss a lower spinal problem located just beyond the intended focus. Similarly, if contrast is required to assess a liver lesion but is not administered, the scan may remain incomplete. Likewise, when a patient with headache, vomiting, or hemiparesis has diffusion-weighted imaging (DWI and ADC) demonstrating an acute infarct. Still, if no vascular sequences are obtained, the study may miss an arterial occlusion—MRA (3D TOF) is often necessary to identify right or left MCA occlusion. Without the appropriate sequences or contrast, MRI or CT brain studies can remain incomplete.
Why incomplete scans can harm patients
When a technologist strictly follows a narrow field of view without adapting to the clinical situation, CT and MRI scan reporting accuracy may suffer. This can lead to delayed treatment, repeated procedures, financial burden, and avoidable anxiety for patients.
The double radiation risk
Returning for a second CT increases cumulative radiation exposure. According to literature cited by the European Society of Radiology, repeated CT examinations can, in some patients, result in cumulative effective doses exceeding 100 mSv. Over time, this may increase long‑term health risks.
Time, cost, and stress
Incomplete scans often require repeat appointments, additional fees, and longer waits for diagnosis. For patients already coping with pain or uncertainty, this can be emotionally and financially draining. A more complete scan initially reduces both the financial and psychological burden.
Real‑world scenarios: when symptoms hide in plain sight
Imaging follows procedural boundaries, but the true source of a patient’s symptoms may lie just beyond those limits. These examples show how missed findings on CT and MRI can occur when protocols are not adjusted in real time.
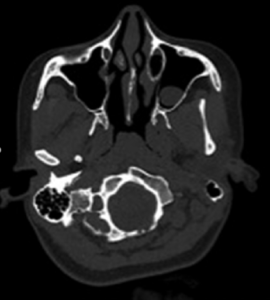
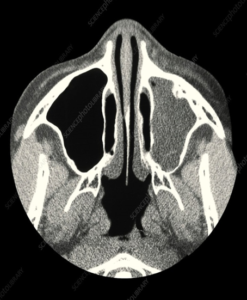
Case 1: Brain pain that starts in the sinuses
A patient presents with severe headache, nausea, and vomiting, and a CT head is ordered. Standard brain CT is centered on the cerebral parenchyma and cranial vault, though the first axial slices often include parts of the facial structures, including the paranasal sinuses. If a left maxillary polyp or significant mucosal thickening is present in those slices, a brain‑only interpretation may miss the true cause. The patient may receive a normal brain report while the sinus disease responsible for the symptoms remains unaddressed.
Better approach: If sinus pathology is suspected, perform a dedicated CT paranasal sinuses (PNS) study.
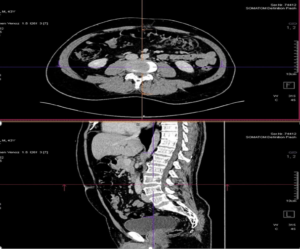
Case 2: Abdominal pain caused by a spinal problem
Referred pain can point attention to the wrong region. A patient with abdominal pain, vomiting, and posterior lumbar discomfort may undergo a non‑contrast CT (NCCT) abdomen. Although the scan evaluates abdominal organs well, the field edge may capture the lower spine. If the spine is not reviewed carefully with multiplanar reconstruction (MPR), important findings such as disc bulges at L4–L5 or L5–S1 may be missed. The abdominal report may appear normal while the actual cause remains hidden.
Better approach: Adjacent structures should also be reviewed, and 3D or multiplanar reconstructions should be used when appropriate.
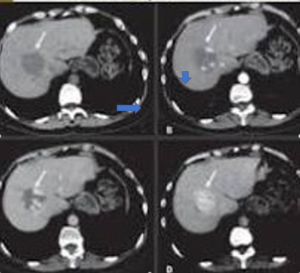
Case 3: A liver lesion that needs contrast
A patient undergoes NCCT abdomen for abdominal discomfort. The unenhanced scan may show a hypodense liver lesion; the question then becomes: can a CT detect cancer? CT can detect suspicious lesions, but without contrast enhancement, it may be impossible to distinguish benign from malignant disease with confidence. If the scan stops there, the diagnosis remains incomplete.
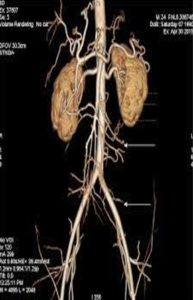
Better approach: Depending on the clinical question, extend the study to a triphasic liver CT, contrast‑enhanced CT (CECT) whole abdomen, or CT angiography for proper characterization.
Case 4: A hidden pulmonary embolism
A patient with prior COVID-19 presents with chest pain, hemoptysis, fatigue, and dyspnea, and HRCT thorax is advised. HRCT is excellent for evaluating lung parenchyma and scarring, but it is non‑contrast and does not adequately assess the pulmonary arteries. If the true problem is a pulmonary embolus, HRCT may miss it entirely. The patient may be sent home with a reassuring report while a dangerous condition persists.
Better approach: If pulmonary embolism is suspected, perform CT pulmonary angiography (CTPA).


Case 5: The hidden stroke in the brain vessels
A patient presents with headache, vomiting, and hemiparesis; an MRI of the brain is performed, and diffusion images may show an acute infarct. However, the vascular cause may remain hidden if arterial imaging is not obtained. If the right middle cerebral artery is occluded, routine MRI sequences alone may not identify the exact vessel occlusion.
Better approach: Add 3D TOF or contrast MRA in the same sitting to identify arterial occlusion.
Case 6: The spine problem behind walking difficulty
A patient presents with neck pain, back pain, nausea, gait disturbance, and urinary difficulty and undergoes an MRI cervical spine. MRI may show spinal abnormalities, but if the symptomatic level lies in the lumbar region—particularly L5–S1—focusing only on the cervical spine will miss the true cause of gait disturbance and urinary symptoms.
Better approach: Expand the protocol to include MRI lumbar spine when clinically indicated.
The Eskag Sanjeevani approach
At Eskag Sanjeevani, we favour a responsive imaging approach rather than an assembly‑line model that can leave patients without answers. Our advanced CT and MRI systems produce high‑resolution images quickly, reducing scan time and radiation exposure on CT while improving diagnostic detail.
If an unexpected abnormality appears during the scan, our protocols allow real‑time adaptation to evaluate it more completely. This helps ensure a more accurate and comprehensive diagnosis in a single visit, avoiding unnecessary repeat scans and their associated radiation and costs.
How to be an empowered patient
Taking an active role in your care improves the chance of a complete diagnosis at the first visit.
- Share your complete medical history and symptom list: Note all symptoms, even those that seem unrelated. Pain can radiate from another region, and a complete picture helps the technologist and radiologist target the study.
- Understand the scope of your scan: Ask which anatomical areas will be covered so you know whether the scan is broad enough to capture the likely source of symptoms.
- Ask about contrast requirements: Some CT and MRI studies need contrast to assess vessels or soft tissues properly. Clarifying this in advance may prevent missed findings.
- Speak up during the procedure: If you recall an important symptom while being positioned, inform the technologist immediately.
- Request a thorough review: It is reasonable to ask whether the team will check adjacent structures and the outer edges of the scan before you leave.
Final thoughts
To reduce the risk of incomplete testing, always share your full symptom history before imaging. If your pain radiates across multiple regions, ask whether adjacent structures should also be reviewed. Choosing an imaging centre that values real‑time adaptability is one of the best ways to reduce missed findings in CT and MRI.
Eskag Sanjeevani uses advanced CT and MRI technology and a proactive diagnostic approach to tailor studies to each patient’s needs. With the right team and clear communication, you can improve the chance of getting a precise answer on your first visit.

Missed diagnoses commonly occur when the scan is limited to a narrow field of view or when MRI sequences are incomplete, and the true cause of symptoms lies outside the scanned area.
A scan may miss a condition if the boundaries are too narrow, the necessary sequences are omitted, or contrast is needed but not used.
Share your complete symptom history, including any radiating pain, so the technologist can adapt the scan if needed.
A repeat CT increases cumulative radiation exposure, adds cost (for both CT and additional MRI sequences), and delays treatment.
Yes. Asking about your symptoms and the scan scope can help the technologist adjust the protocol in real time.