
10-Minute CT Angiogram: Detect Blockages Without Surgery
Every year, thousands of people suffer a heart attack without ever experiencing a warning symptom, because the arterial disease driving it went undetected for years. For anyone living with chest discomfort, unexplained breathlessness, or multiple cardiovascular risk factors, that reality is not abstract. Coronary artery disease does not announce itself until it reaches a critical threshold, and by then, the clinical options narrow considerably. A CT angiogram changes that equation by detecting blockages, plaque composition, and arterial narrowing non-invasively, before a cardiac event forces the decision.
In this blog, we break down exactly how a CT coronary angiogram works, what it detects, how it compares to conventional angiography, and who should consider getting one.
Key Takeaways:
- Computed Tomography Coronary Angiography (CTCA) carries 95–99% sensitivity for detecting coronary blockages, among the highest of any non-invasive cardiac test.
- A normal CTCA result has an 89% negative predictive value, reliably ruling out significant coronary artery disease.
- CTCA detects vulnerable plaque that stress tests miss, enabling intervention before a cardiac event occurs.
Quick Answer: A CT coronary angiogram is a non-invasive 10-minute scan that detects coronary artery blockages, plaque composition, and stenosis severity with 95-99% sensitivity, without catheter insertion, sedation, or hospital admission.
Quick Links
- What Is a CT Coronary Angiogram?
- How Is the CT Coronary Angiogram Procedure Performed?
- What Does a CT Angiogram Detect: And How Accurately?
- CT Coronary Angiogram vs Conventional Angiogram: Key Differences
- Who Should Get a CT Coronary Angiogram?
- Understanding Your CT Angiogram Results: What the Report Means
- Why Choose Eskag Sanjeevani for CT Angiogram
What Is a CT Coronary Angiogram?
A coronary CT angiography (CTA) is a non-invasive imaging test that visualises the coronary arteries using X-rays and intravenous contrast dye. Unlike a standard CT scan, CTCA uses ECG-gating technology to synchronise image acquisition with the heartbeat, eliminating motion blur entirely. It produces high-resolution, three-dimensional maps of coronary vasculature, identifying arterial narrowing, calcified and non-calcified plaque, and structural abnormalities before symptoms develop.
Research confirms that CTCA has a sensitivity of 95-99% in detecting significant coronary artery blockages, making it one of cardiology’s most reliable non-invasive diagnostic tools [1]. Crucially, it detects plaque accumulation years before a cardiac event, a window that conventional testing often misses. The European Society of Cardiology recognised this in its 2019 guidelines, designating CTCA as the first-line investigation for stable chest pain. Results are reported using the CAD-RADS scoring system, grading stenosis severity from 0 to 5 for standardised clinical decision-making.
How Is the CT Coronary Angiogram Procedure Performed?
A coronary CT angiogram requires precise clinical preparation to deliver diagnostically reliable images. The 10-minute scan is only one part of a 45-60-minute appointment.
- Heart rate optimisation. If resting heart rate exceeds 65-70 bpm, oral or IV beta-blockers are administered [2]. Sublingual nitroglycerin is given immediately before scanning to dilate the coronary arteries and improve the distal vessel visualisation.
- IV contrast and ECG gating. Iodinated contrast dye is injected intravenously using a dual-head power injector. ECG electrodes time image acquisition to end-diastole, the cardiac cycle’s most stable phase, eliminating motion artefact.
- The patient holds their breath for 10-15 seconds while a 64-slice minimum CT scanner captures hundreds of cross-sectional images in a single acquisition.
- Raw data is post-processed into 3D coronary maps. Stenosis in each arterial segment is graded using the CAD-RADS scoring system, from 0 (no plaque) to 5 (total occlusion) [3].
- Same-day discharge follows. Patients must hydrate post-procedure for contrast clearance. Diabetics on metformin must withhold it for 48 hours to prevent contrast-induced lactic acidosis.
What Does a CT Angiogram Detect: And How Accurately?
CTCA goes beyond confirming blockages; it characterises the composition and haemodynamic significance of coronary artery disease in detail, and no other non-invasive test currently matches.
- CTCA differentiates calcified stable plaque from soft, lipid-rich non-calcified plaque, the latter of which is significantly more prone to rupture and acute coronary events, even without severe stenosis.
- CTCA has a negative predictive value of 89%, reliably excluding significant CAD in low- to intermediate-risk patients and avoiding unnecessary invasive procedures.
- For intermediate stenoses of 30–90%, FFR-CT uses computational fluid dynamics applied to CTCA data to determine whether narrowing is causing actual ischaemia, without additional invasive testing.
- Because CTCA images the entire chest, it simultaneously identifies pulmonary embolism, aortic dissection, pericardial effusion, and lung nodules, conditions that otherwise require separate investigations.
- Accuracy drops in heavily calcified arteries and existing stents, where the calcium blooming artefact can exaggerate stenosis severity and generate false positives.
Also read: Angiography vs Angioplasty: Understanding the Key Differences in Heart Procedures
CT Coronary Angiogram vs Conventional Angiogram: Key Differences
A cardiac CT scan and a conventional angiogram both visualise coronary arteries, but they differ fundamentally in invasiveness, clinical application, and what each can and cannot achieve.
Here is a tabular representation to understand the difference between the two:
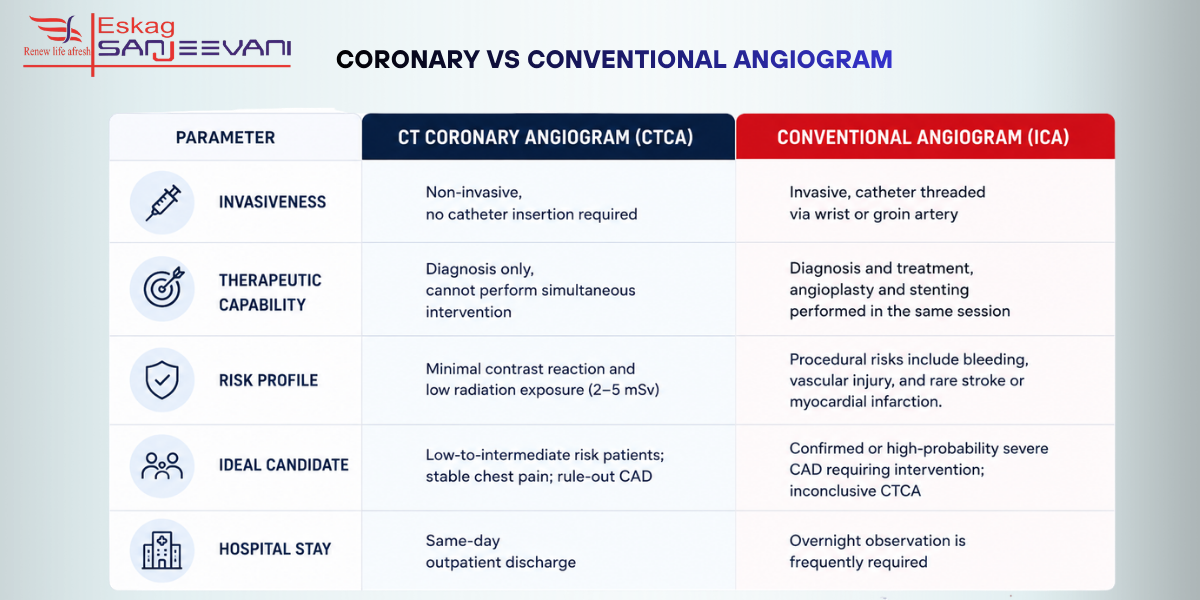
| Parameter | CT Coronary Angiogram (CTCA) | Conventional Angiogram (ICA) |
| Invasiveness | Non-invasive, no catheter insertion required | Invasive, catheter threaded via wrist or groin artery |
| Therapeutic capability | Diagnosis only, cannot perform simultaneous intervention | Diagnosis and treatment, angioplasty and stenting performed in the same session |
| Risk profile | Minimal contrast reaction and low radiation exposure (2–5 mSv) | Procedural risks include bleeding, vascular injury, and rare stroke or myocardial infarction. |
| Ideal candidate | Low-to-intermediate risk patients; stable chest pain; rule-out CAD | Confirmed or high-probability severe CAD requiring intervention; inconclusive CTCA |
| Hospital stay | Same-day outpatient discharge | Overnight observation is frequently required |
Clinical nuance: Conventional angiography remains the gold standard when revascularisation, stenting, or bypass is anticipated.
Who Should Get a CT Coronary Angiogram?
CTCA is appropriate for symptomatic patients with chest pain and no established CAD diagnosis, specifically those with low-to-intermediate pre-test probability, where invasive angiography is not yet clinically justified. Beyond chest pain, validated indications include new-onset heart attack without prior CAD, inconclusive stress test results, and preoperative coronary assessment before non-cardiac surgery. Asymptomatic individuals over 40 with multiple converging risk factors, hypertension, dyslipidaemia, diabetes, active smoking, or a first-degree family history of premature CAD, represent a population where early CTCA-based detection meaningfully changes long-term management.
Conversely, uncontrolled atrial fibrillation, severe renal impairment exceeding serum creatinine of 1.8 mg/dL, and prior anaphylaxis to iodinated contrast are recognised contraindications. In each of these cases, the clinical decision is not simply whether CTCA is available; it is whether the pre-test clinical profile makes the result actionable.
Understanding Your CT Angiogram Results: What the Report Means
A CT angiogram report uses the CAD-RADS scoring system to systematically grade the severity of coronary artery disease; each score carries a specific clinical implication and a recommended next step.
| CAD-RADS Score | Stenosis Severity | What It Means | Recommended Next Step |
| CAD-RADS 0 | No plaque detected | Coronary arteries are clear, no evidence of atherosclerosis | No further cardiac workup required; reassess if symptoms change |
| CAD-RADS 1 | Minimal stenosis (1–24%) | Early plaque present, but not flow-limiting | Lifestyle modification: preventive cardiology review |
| CAD-RADS 2 | Mild stenosis (25–49%) | Plaque present; no significant arterial narrowing | Medical management, statins, antihypertensives; periodic monitoring |
| CAD-RADS 3 | Moderate stenosis (50–69%) | Potentially flow-limiting; clinical significance uncertain | Functional assessment recommended, stress testing or FFR-CT |
| CAD-RADS 4A | Severe stenosis (70–99%), single vessel | Haemodynamically significant narrowing, high likelihood of ischaemia | Invasive coronary angiography referral; revascularisation planning |
| CAD-RADS 4B | Severe stenosis, left main or three-vessel disease | High-risk anatomy carries significant mortality implications | Urgent cardiology review; surgical revascularisation evaluation |
| CAD-RADS 5 | Total occlusion (100%) | Complete vessel blockage, chronic or acute | Immediate cardiology intervention; viability assessment required |
| CAD-RADS N | Non-diagnostic scan | Image quality insufficient for accurate interpretation | Repeat CTCA or proceed to invasive angiography |
Beyond stenosis grading, the report also documents the coronary calcium score, a separate but complementary marker of overall atherosclerotic burden. A high calcium score in the absence of obstructive stenosis still carries independent prognostic significance and warrants aggressive risk factor modification.
Why Choose Eskag Sanjeevani for CT Angiogram
Accurate cardiac diagnosis depends as much on the clinical team interpreting the results as on the technology performing the scan. At Eskag Sanjeevani, CT coronary angiograms are reported by experienced cardiologists and radiologists working in a multidisciplinary framework, ensuring CAD-RADS findings translate directly into a structured, individualised management plan rather than an isolated report. For patients in Kolkata navigating chest pain, inconclusive stress tests, or elevated cardiovascular risk, having a diagnosis and specialist cardiology review under one roof meaningfully reduces the gap between detection and clinical action.
Final Thoughts
Coronary artery disease remains the leading cause of preventable death globally, and its most dangerous characteristic is how silently it progresses. A CT angiogram offers a clinically validated, non-invasive opportunity to detect progression early, at a stage when medical management, lifestyle interventions, and close monitoring can meaningfully alter the outcome. If you have persistent chest discomfort, an inconclusive stress test, or multiple converging risk factors, do not defer cardiac evaluation; initiate a conversation with a cardiologist and ask specifically whether CTCA is appropriate for your clinical profile. Understanding your CAD-RADS score is not just diagnostic information; it is a roadmap for every clinical decision that follows. The cardiology team at Eskag Sanjeevani is equipped to guide the process from scan to a structured management plan, without unnecessary delay.

Microbiologist with over 2 years of experience in medical writing, specialising in evidence-based healthcare content.

Clinical experience in diagnosis, treatment, and evidence-based patient care across a range of conditions.
References
- Ramjattan, N.A., Lala, V., Kousa, O. and Makaryus, A.N. (2019). Coronary CT Angiography. [online]
- Prat-Gonzalez, S., Sanz, J. and Garcia, M.J. (2008). Cardiac CT: Indications and Limitations. Journal of Nuclear Medicine Technology, 36(1), pp.18–24.
- Lee MY, Han B, Jenkins C, Xing L, Suh TS. A depth-sensing technique on 3D-printed compensator for total body irradiation patient measurement and treatment planning. Med Phys. 2016 Nov;43(11):6137. doi: 10.1118/1.4964452. PMID: 27806603; PMCID: PMC5085972.
No. CTCA is non-invasive, no catheter, no sedation, no overnight stay. A conventional angiogram threads a catheter through the wrist or groin and can perform simultaneous stenting. CTCA diagnoses, conventional angiography diagnoses and treats. When revascularisation is already anticipated, conventional angiography is the appropriate choice.
The scan takes approximately 10 minutes. The full appointment — heart rate optimisation, contrast preparation, ECG setup, and post-procedure monitoring — spans 45–60 minutes. Same-day discharge follows in virtually all cases, with results available within 24–48 hours.
Yes. CTCA identifies lipid-rich, non-calcified plaque at high risk of rupture, even without symptoms or severe stenosis. Stress tests only detect ischaemia beyond 70% stenosis. CTCA detects disease at earlier, more treatable stages, making it a genuinely preventive tool rather than a reactive one.
Not without careful assessment. Iodinated contrast carries a risk of nephropathy in patients with compromised renal function. Patients with serum creatinine exceeding 1.8 mg/dL are generally unsuitable. Diabetics on metformin must discontinue it 48 hours before and after the procedure. Alternative investigations should be considered in significant renal impairment.