
Direct Anterior Approach: Future of Total Hip Replacement
Hip arthritis and joint deterioration affect millions worldwide, severely limiting mobility and diminishing quality of life through persistent pain and functional disability. Traditional hip replacement surgery has transformed countless lives, yet the selection of surgical approaches significantly impacts recovery speed, complication rates, and long-term outcomes for patients. The direct anterior approach represents a paradigm shift in total hip arthroplasty, utilising muscle-sparing techniques that preserve anatomical structures rather than cutting through them. This innovative surgical method offers faster recovery, reduced dislocation risk, and immediate unrestricted movement compared to conventional posterior or lateral approaches.
In this blog, we’ll explore how direct anterior hip replacement works, compare it with traditional techniques, examine evidence-based benefits and limitations, and guide you toward making informed decisions about your joint replacement surgery.
Key Takeaways:
- The direct anterior approach accesses the hip through natural muscle planes without cutting any tissue, enabling immediate, unrestricted postoperative mobility.
- Recovery occurs significantly faster with shorter hospital stays, reduced pain, and lower dislocation rates compared to traditional posterior approaches.
- Surgeon experience matters critically; the learning curve requires 50-100 cases before complication rates normalise to optimal levels.
Quick Answer: The direct anterior approach to hip replacement is a muscle-sparing surgical technique that accesses the hip joint from the front of the body, between natural tissue planes, avoiding muscle cutting entirely.
Quick Links
- What Is the Direct Anterior Approach to the Hip?
- How Is Direct Anterior Total Hip Arthroplasty Performed?
- Direct Anterior Approach vs. Posterior vs. Lateral: A Clinical Comparison
- Benefits of Direct Anterior Hip Replacement
- Risks and Limitations: An Honest Clinical Assessment
- Why Choose Eskag Sanjeevani for Expert Orthopaedic Care
What Is the Direct Anterior Approach to the Hip?
For decades, surgeons accessed the hip joint by cutting through the gluteal muscles from the back or side. The direct anterior approach changes that entirely. Instead of dividing muscle, the surgeon works through a natural anatomical corridor. The Smith-Petersen interval is between the sartorius and the tensor fasciae latae at the front of the hip. No muscle is cut, detached, or required to heal post-operatively.
Here is what defines it clinically:
- Truly muscle-sparing technique: Operates within an intramuscular plane, preserving the integrity of all surrounding soft tissues.
- Smaller anterior incision: 3-4 inches at the front of the hip versus up to 12 inches with traditional posterior approaches.
- Intraoperative fluoroscopy-guided: Real-time X-ray confirms accurate implant positioning, leg length, and hip offset during surgery.
- No post-operative hip precautions: Posterior capsule remains intact, eliminating the movement restrictions mandatory after posterior approach surgery.
- Specialised technique: Requires dedicated instruments, a traction table, and a surgeon with specific DAA training; complication rates are demonstrably higher during early learning-curve cases.
Now, let’s understand how direct anterior total hip arthroplasty is performed.
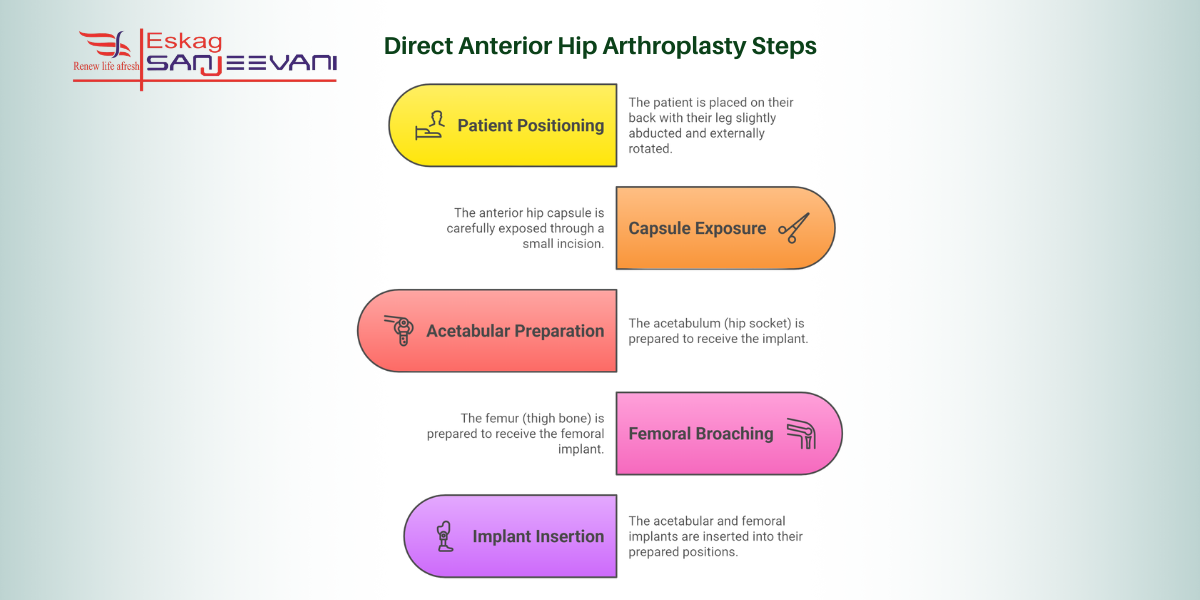
How Is Direct Anterior Total Hip Arthroplasty Performed?
The direct anterior approach to the hip utilises specialised surgical technique and intraoperative fluoroscopy to replace the arthritic joint while preserving the integrity of the surrounding muscles by maintaining anatomical tissue planes.
Here is a comprehensive breakdown of the process:
1. Patient Positioning
The patient lies supine on a specialised traction table or a standard operating table, with the legs secured in positioning boots. A 3-4 inch oblique incision is made approximately 2 cm posterior and 2 cm distal to the anterior superior iliac spine. Dissection proceeds through subcutaneous layers to the tensor fasciae latae fascia, which is opened to access the Smith-Petersen intermuscular interval between the sartorius and the tensor fasciae latae muscles without cutting either structure.
2. Capsule Exposure
After retracting muscles laterally and medially, surgeons visualise the anterior hip capsule. An anterior capsulotomy opens the joint, and capsular flaps are tagged with sutures for anatomical repair during closure. Based on preoperative templating, a femoral neck osteotomy removes the arthritic femoral head, providing initial acetabular access.
3. Acetabular Preparation
Retractors expose the socket after osteophytes and labral tissue are removed. Sequential hemispheric reamers of progressively increasing diameter reshape the acetabulum. Intraoperative fluoroscopy confirms proper component positioning, with acetabular inclination at 40-45 degrees and anteversion at 15-25 degrees to optimise stability. Research demonstrates 100% cup alignment success within the safe zone after completing the initial 50-case learning curve.
4. Femoral Broaching
The posterior capsule is released posterolateral to the greater trochanter, allowing femoral elevation with specialised retractors. Sequential broaching with progressively larger rasps prepares the femoral canal until optimal press-fit stability is achieved. Mean surgical time improves significantly from 82.5 minutes during the first 50 cases to 72.0 minutes in the second 50 cases as surgeon experience increases [1].
5. Implant Insertion
The metal acetabular cup is impacted and supplemented with screws if needed. A polyethene liner locks into the cup, the femoral stem is inserted, and a ceramic or metal head attaches. After hip reduction, thorough irrigation precedes layered closure with absorbable sutures.
Suggested read: Kolkata’s Trusted Team for Joint Replacement Surgery with Advanced Care.
Direct Anterior Approach vs. Posterior vs. Lateral: A Clinical Comparison
The direct anterior approach differs fundamentally from posterior and lateral approaches in surgical technique, muscle disruption, and postoperative outcomes.
Here’s a tabular representation to understand the difference between the three processes:
| Parameter | Direct Anterior | Posterior | Lateral |
| Muscle Cutting | No muscles cut or detached | Gluteus maximus split; external rotators detached | Gluteus medius/minimus split or detached |
| Dislocation Rate | 0.77-0.84% lowest reported [2] | 1.82% higher risk [3] | 0.43-0.70% intermediate risk |
| Hospital Stay | 7 days shorter average | 10 days standard duration | 8-9 days moderate duration |
| Learning Curve | 50-100 cases steep curve | Familiar, well-established technique | Established; moderate learning curve |
| Postoperative Pain | Lower early pain scores | Moderate posterior discomfort | Higher lateral hip pain |
Next, with a proper understanding of the process, let’s explore the benefits of direct anterior hip replacement.
Benefits of Direct Anterior Hip Replacement
The direct anterior approach offers distinct clinical advantages, including muscle preservation, immediate unrestricted mobility, and accelerated functional recovery, compared with traditional approaches.
- No muscles are cut, split, or detached during the procedure. Patients can sleep, sit, and move without hip precautions starting on day 1 postoperatively, whereas patients with a posterior approach face 6 weeks of strict movement restrictions.
- Posterior capsule preservation maintains critical anatomical stabilisers, resulting in dislocation rates of 0.77-0.84% compared with 1.82% with posterior approaches. A meta-analysis demonstrates a 68% lower risk of dislocation (RR 0.32, P<0.001).
- Patients demonstrate a quicker return to normal gait, shorter hospital stays (averaging 7 days versus 10 days), and earlier achievement of physical therapy milestones.
- Less postoperative pain indicates minimal surgical trauma to surrounding tissues. Lower creatine kinase and C-reactive protein levels demonstrate objectively less muscle damage.
- Real-time fluoroscopic guidance achieves 100% cup alignment within safe zones after learning curve completion
However, there are certain risks associated with the surgical process that you must be aware of.
Risks and Limitations: An Honest Clinical Assessment
Direct anterior approach hip replacement requires specialised training and careful patient selection due to specific technical challenges and complication risks not encountered with traditional approaches.
- The first several dozen cases carry higher complication rates, including intraoperative fractures, component malposition, increased operative time, and elevated blood loss, requiring careful patient selection during transition periods.
- Persistent symptoms occasionally affect long-term satisfaction, with diabetes, obesity, and significant postoperative inflammation increasing the risk of permanent nerve-related complications.
- Limited surgical exposure in heavier patients also prolongs operative time and increases bleeding, making alternative approaches more appropriate for severely obese individuals.
- Osteoporotic bone is common among elderly patients, increasing fracture susceptibility, though experienced surgeons demonstrate significantly lower rates through refined techniques and judicious patient selection.
- Abnormal bone structure, prior hardware, excessive scar tissue, or muscular contractures necessitate alternative approaches providing superior visualisation and broader surgical access.
Why Choose Eskag Sanjeevani for Expert Orthopaedic Care
Eskag Sanjeevani Hospital provides comprehensive orthopaedic services through highly experienced surgeons specialising in advanced hip and knee joint replacement procedures. The Orthopaedic department offers state-of-the-art facilities, including fully equipped operating theatres, intensive care units for pre- and postoperative monitoring, and dedicated rehabilitation services ensuring optimal recovery outcomes.
Our team of the best orthopaedic surgeons in Kolkata utilises the latest surgical techniques for total hip and knee replacements, arthroscopy, ligament repair, and complex trauma management, with a proven track record. With multiple units across Baghbazar, Baranagar, and Khardah, patients have access to convenient, affordable, quality orthopaedic care supported by multidisciplinary teams including anesthesiologists, physiotherapists, and specialised nursing staff, ensuring comprehensive treatment from diagnosis through complete recovery.
Final Thoughts
If persistent hip pain limits your daily activities despite conservative treatments, total hip arthroplasty via the direct anterior approach may effectively restore your mobility and quality of life. Consult with experienced orthopaedic surgeons who have completed the learning curve and perform this technique regularly to ensure optimal outcomes and minimise complications. Research your surgeon’s training, case volume, and complication rates before committing to surgery, as expertise directly correlates with successful results.
Eskag Sanjeevani Hospitals offer comprehensive orthopaedic services with multidisciplinary support teams ensuring coordinated care from preoperative planning through complete rehabilitation. Remember that while the direct anterior approach offers distinct advantages, individual anatomical factors, body habitus, and medical history determine candidacy. It makes personalised surgical planning with your orthopaedic team essential for achieving the best possible outcome for your specific situation.

References
- Nakamura J, Hagiwara S, Orita S, Akagi R, Suzuki T, Suzuki M, Takahashi K, Ohtori S. Direct anterior approach for total hip arthroplasty with a novel mobile traction table -a prospective cohort study. BMC Musculoskelet Disord. 2017 Jan 31;18(1):49. doi: 10.1186/s12891-017-1427-2. PMID: 28137262; PMCID: PMC5282798.
- Huang XT, Liu DG, Jia B, Xu YX. Comparisons between Direct Anterior Approach and Lateral Approach for Primary Total Hip Arthroplasty in Postoperative Orthopaedic Complications: A Systematic Review and Meta-Analysis. Orthop Surg. 2021 Aug;13(6):1707-1720. doi: 10.1111/os.13101. Epub 2021 Aug 5. PMID: 34351056; PMCID: PMC8523754.
- Xu, W., Lao, J., Liu, J., Zhang, Z., Wan, X., Chen, Z., Huang, X., Chen, N. and Xu, Y. (2025). Comparison of direct anterior vs. posterior approach in primary total hip arthroplasty: a systematic review and meta-analysis on enhanced recovery after surgery. Frontiers in Surgery, 12, pp.1586187–1586187.
Most patients resume light activities within one to two weeks after direct anterior hip replacement. Full recovery typically occurs within six to twelve weeks, compared with three to six months with traditional approaches.
A body mass index above 35 presents technical challenges, including limited exposure and elevated risks of wound complications. Surgeons typically recommend alternative approaches for significant obesity, though experienced specialists may perform it in selected cases.
Hip precautions are movement restrictions that avoid bending beyond 90 degrees or crossing the legs to prevent dislocation. These become unnecessary after the direct anterior approach because the posterior capsule and stabilising muscles remain intact.
Ask potential surgeons about their annual case volume, years of experience performing the technique, and complication rates. Seek surgeons who have completed at least 100 cases, as complication rates normalise after this threshold.
The direct anterior approach is primarily for straightforward primary replacements with normal anatomy. Complex revisions, severe dysplasia, or extensive scar tissue typically require posterior or lateral approaches, providing superior visualisation.